

HOW CAN WE ACHIEVE A GOOD TISSUE MANAGEMENT WITHOUT THE REST OF THE HASSLE THAT GOES WITH IT IN ITS IMPLEMENTATION?
One of the most challenging step as we practice Prosthodontics and other dental treatments especially those that require impression taking is the management of the gingival tissue prior to this procedure. Generally, tissue management is much done for the need of displacing the gingival tissue away from the prepared tooth with the use of a retraction cord or paste. This way the margins and finish line we need to expose is achieved, and this can also be accomplished with the combination of a solution that can provide hemostasis when the gingival tissues starts to bleed.
Whether or not the impression is made conventionally with impression material or with a digital impression technique, all the tooth margins must be captured to assure an excellent marginal fit of a lab fabricated restoration. So, to assists us in doing exactly that, here are some of the tips on how we can do this and receive a truly great fit on the final restorations done by the lab and minimize or no redo because we provided our laboratory technicians the accurate replication needed during the lab fabricated procedures.
KNOW YOUR CORD
A retraction cord is a cord made of cotton often used to displace tissue during tooth preparation. It comes in different diameters and designs (such as braided and knitted cord)
DIFFERENT RETRACTION CORD DESIGNS:
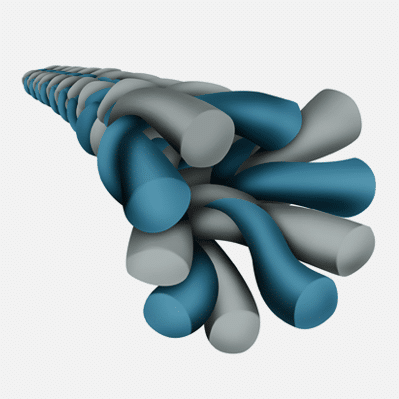
Braided Cord
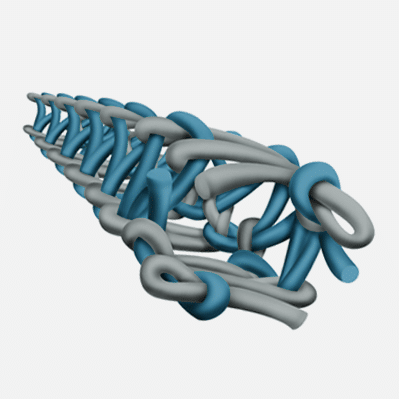
Knitted Cord
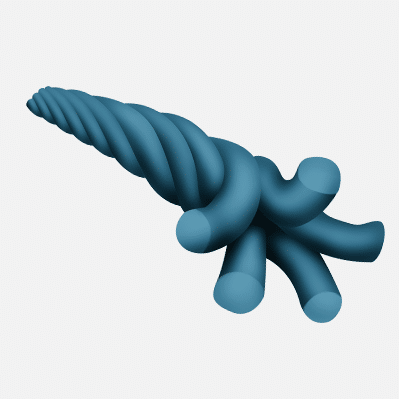
Twisted Cord
A study was published that knitted cord design has its specific advantages to other cord designs. However, in reality, to sum it all up, there's no critical clinical advantage/s which cord should be used by dentists to achieve successful displacement of gingiva. It’s really mainly on the dentist's preference as to what cord design that gives the dentist the ease of use to place it that's important.
Each cord has a variety of diameters and sizes to allow for ease of placement in tighter and healthier gingival sulcuses.
000 - It is used usually for upper and lower anterior teeth or teeth with thin and sensitive gingiva. Also used as the lower cord during double-cord technique
00 - It is used usually for upper and lower anterior teeth . Also used as the lower cord during double-cord technique. Can be used as a guide during preparation and fixing of veneers.
0 - It is used usually for upper and lower anterior teeth. Also used as the lower cord during double-cord technique. Used to isolate gingiva during restoration of the classes III, IV and V.
1 - It is used usually for upper anterior teeth and premolar. Can be used to isolate the gingiva during pre- preparation of crown.
2 - It is used mainly for upper cord with the double-cord technique. Also used in gingival retraction pf premolar and molar areas / Protection during pre-preparation of premolar during crown reduction
3 - Mainly for molars or areas with thicker gingiva. Should be used with caution as it can cause tissue trauma.
NOTES: In some studies by Dragoo and Williams discussed that placing retraction cord while finishing your preparation can produce minimal gingival lesions and the best tissue results for operative procedures.)
When handling retraction cord it is important to remember to use latex-free gloves because contamination of the cord with latex can have a deleterious effect on the setting of the VPS impression materials. This is important when a light body material is placed first into the sulcus. If it does not cure completely, it can result in inaccuracies or tearing of the fine gingival margin within the impression.
USING THE RIGHT INSTRUMENT
In choosing the right instrument you can save yourself the trouble of damaging the gingiva or in inserting the retraction cord. Usually, the end of the cord packer are usually thin enough to placed in the gingival sulcus without damaging the tissue and causing any bleeding.
There are 2 types of cord packers: 45 degrees and 90 degrees. The angulation of the instrument helps in the orientation for the placement.
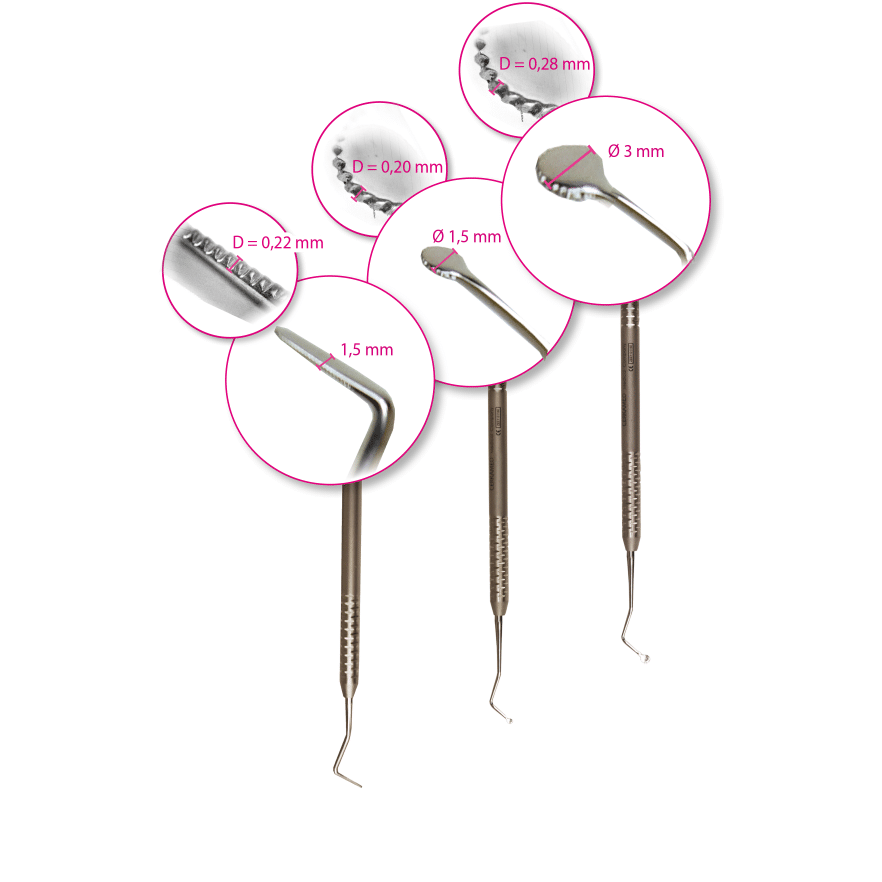
Most clinicians prefers a non-serrated instrument easier as the cord won’t pull back out of the sulcus. Design of the instrument is limited to the manufacturer, but many dentists utilize two different instruments depending on the tooth location. Thin, flat instruments for anterior tissue (which tends to be thinner and tighter) works quite well, and rounder serrated or non-serrated work better for posterior teeth
It is recommended in packing of the retraction cord, that it should be started in the inter-proximal area. This can be done with the help of a periodontal probe and gentle pressure as the inter-proximal gingival is thin and delicate, with minimal depth of gingival sulcus. There are two broadly used techniques for packing retraction cord in the gingival sulcus depending on the clinical situation, the health of the gingival tissues, the depth of the gingival sulcus and the placement of the margin of the preparation on the tooth structure.
KNOW YOUR CHEMISTRIES: ASTRINGENTS AND VASOCONSTRICTORS
There are different chemicals used for local hemostasis during soft tissue management: Astringents and Hemostatic agents.
Astringents causes a contraction-retraction of the tissues while the Hemostatic agents constrict blood flow through coagulation. Usually they are impregnated to a mechanical component (retraction cord) to offer better sulcus displacement
The effect of astringent agents (e.g. ferrous sulfate, aluminum chloride) is based on their ability for precipitation of proteins. Ferrous Salt Compounds: By local precipitation of proteins in the blood, ferrous sulfate causes obstruction of the blood vessels. Aluminum Salt Compounds: The precipitation of proteins results in a slight tissue shrinkage.

When used for duration of less than 10 minutes, they cause minimal tissue damage. These chemicals can interfere with the surface detail of the impression material and with the dentin surface, so thoroughly cleaning the dentin before using a resin bonded cement is recommended.
When using epinephrine impregnated cord, it should be considered to know if the patient has any history of any cardio vascular diseases. Epinephrine can cause elevated heart rate, blood pressure (especially if placed into bleeding tissues) or worst over dosage due cumulative effect in the body.
But, if you are still to use them, there are a lot of studies that show there are no clinical benefit in gingival retraction with using this.
LEARN ABOUT ALTERNATIVE OPTION: CORDLESS RETRACTION
There are a lot of alternative to retraction cords, these are various pastes and gels for soft tissue management that's available in the market. They are great to work with as they give excellent retraction that is non-traumatic and non-invasive. Expasyl, Traxodent and GingiTrac are probably the most popular ones.
Retraction pastes and gels are usually made from a viscous paste of diatomaceous clay that contains astringent component (often aluminum chloride 15 %) which is responsible for the hemostatic effect, and a component for the tissue displacement (often kaolin, that absorbs sulcus fluid and expands). Usually the pastes are introduced into the sulcus with a blunt cannula and rinsed out after a certain application time (depending on the manufacturers instructions).

One should always keep in mind to try the compatibility of the retraction gel or paste with the impression material used during these procedure to avoid any unnecessary shrinkage.
THE STYLE OF DOUBLE-CORD TECHNIQUE
The double cord is likely the most popular and predictable method of tissue displacement. The name of the technique is descriptive in nature in that two distinct cords usually of differing sizes are actually used.
Tips in Doing Double Cord Technique:
➢Evaluate the health of the gingiva, depth of the sulcus and the thickness of the gingiva.
➢Choose the appropriate cord to use on the tooth. If there is minimal sulcus depth, it will only accommodate a single cord technique and probably only a thin cord. A deep sulcus can accommodates a double cord technique (thin in first followed by a wider diameter).
➢Using a cotton plier, submerge the cords into the hemostatic solution for atleast 2 mins to fully coat it. Place the cord on top of a clean gauze to remove excess solution.
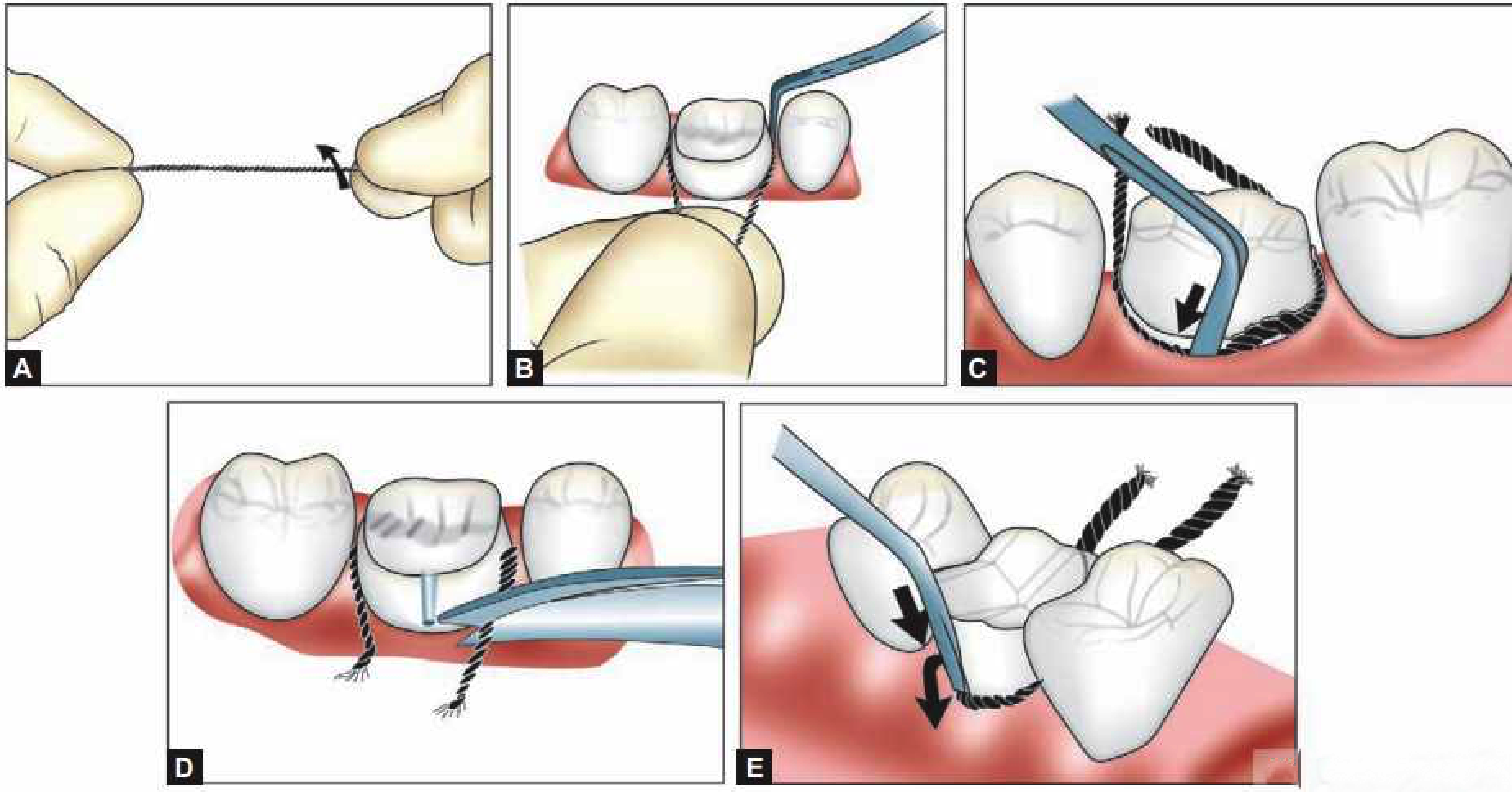
➢Twist the first cord very tightly. Pack around the preparation with a cord packer. Avoid using explorer as it may puncture the gingiva. Overlap the cord slightly and gently tuck it down beneath the shoulder of the prep. In this way, the cord will unwind and force the tissue to displace laterally away from the tooth.
➢Repeat process with the second cord. Again the cord will unwind slightly and force the tissue laterally.
➢Cover preparation with a folded 2×2 gauze, ask patient to bite on this to prevent wash out of the hemostatic solution and to avoid the negative taste
➢Leave the cords in place three to five minutes.
➢Remove gauze, remove secondary cord, rinse and lightly dry, evaluate tissue displacement and hemostasis, reapply hemostatic solution and gently scrub the widened sulcus. Gently wash the cord with water so it won’t grab and tear any tissues when it is removed.
➢Once the cord is removed, the retraction is maintained for 30 seconds. Be prepared to begin immediate syringing of your impression material.
CONCLUSION
The longevity and esthetics of restorations significantly depends on the quality and detail of the impression. Retraction cords play an important as they are a great tool in displacing the gingiva and the initial preparation done prior to taking impression. In combination with other chemicals, retraction cords can control blood and sulcular fluid and protection from the soft tissues. They can also be used as a protection of the margin during finishing of tooth preparations. In familiarizing ourselves with these materials we can avoid the difficulties that we may possibly encounter during the implementation of tissue management.
CONTRIBUTOR:
Dr. Bryan Anduiza - Writer
Dr. Mary Jean Villanueva - Editor










