
ABSTRACT
The frequency of separation of NiTi rotary instruments has increased with the increasing use of these instruments, and this error may result from inadequate experience of using these instruments. This iatrogenic error can complicate root canal treatment, and special experience is required to manage this problem. This case report describes the management of the separation of an F3 instrument from a ProTaper NiTi rotary system. A 30-year-old man was referred to the College of Dentistry, Taibah University (Saudi Arabia) with an intracanal separated NiTi rotary instrument (F3 of the ProTaper system; Dentsply Maillefer, Ballaigues, Switzerland) in the canal of the maxillary right canine. The separated instrument was removed by using the modified hollow tube–based extractor system. The present case revealed that sometimes a simple method can be an effective alternative of a professional method; using NiTi rotary instruments with strict adherence is important for the prevention of instrument separation.
INTRODUCTION
In recent years, nickel-titanium (NiTi) rotary instruments have been widely used for cleaning and shaping of the root canal system.1 These instruments have many unique features such as a great taper, a novel blade design, and higher elasticity.2 In addition, these instruments keep the original shape of the canal and cause less procedural accidents such as ledge.3,4 Despite all these advantages, separation of NiTi rotary instruments remains a common problem of concern to many practitioners.5 The NiTi rotary instruments are more susceptible to separation compared to stainless steel hand instruments.6 The prevalence of separation of NiTi rotary instruments ranges from 0.5% to 5%.2 The presence of an intracanal-impacted NiTi-separated fragment may lead to undesirable results and failure of non-surgical root canal therapy, in addition to causing anxiety for the patient.7 All the aforementioned reasons increased the interest regarding removal of intracanal separated NiTi rotary instruments and led to new studies on techniques to remove separated instruments.2 There is no single method for treating endodontic cases with NiTi rotary instrument separation;8 there are different techniques to manage this problem, and these techniques include use of ultrasonic tips, endodontic forceps, endodontic files, and hollow tube–based extractor systems.9
The present case report describes the removal of a large separated NiTi endodontic instrument by using the modified hollow tube–based extractor system.
CASE REPORT
A 30-year-old male patient was referred to the endodontic specialty clinic at the College of Dentistry, Taibah University (Saudi Arabia) with an intracanal separated NiTi rotary instrument (F3 of the ProTaper system; Dentsply Maillefer, Ballaigues, Switzerland) in the canal of the maxillary right canine (#13). A root canal retreatment had been initiated previously in a private general dental practice before referral for separation of an F3 ProTaper instrument, which was used during the removal of old root canal obturation material. The medical history of the patient was noncontributory. Diagnostic radiography revealed that the separated instrument extended along the root canal to the apical foramen of the canine, which had a metal ceramic crown (Figure 1(a)). Local anesthesia was administered with 36 mg of lidocaine and 0.018 mg of epinephrine, the metal ceramic crown was sectioned with diamond and carbide burs to facilitate treatment procedures, and then, the tooth was isolated by a rubber dam. A subsequent diagnostic radiographic examination revealed another small separated instrument in the pulp chamber (Figure 1(b)); the access cavity was reevaluated, but there was no need to modify it. Several attempts were made to extract the separated instrument (F3) by using the ultrasonic tip ET25 (SATELEC, A company of the ACTEON Group, France) under magnification with a Leica M320 dental microscope (Leica Microsystems, Wetzlar, Germany); however, the F3 instrument remained firmly fixed and could not be removed. Therefore, the use of another technique was attempted. A tool modified from a hollow tube–based extractor system was used with an etching needle and a K file size 40 (Dentsply Maillefer, Ballaigues, Switzerland) as the extraction device (Figure 2(a)). The etching needle was inserted into the canal and interlocked with the separated instrument, and then, a K file size 40 was inserted into the needle lumen, which shackled the separated instrument (Figure 2(b)). After three attempts to withdraw the separated instrument, the instrument was removed from the canal (Figure 3(a)). The length of the fragment was approximately 16 mm (Figure 3(b)), and then, the small separated instrument in the pulp chamber was removed by using an ultrasonic tip. Cleaning and shaping of the canal were completed by using a new F3 instrument from the ProTaper universal NiTi system, and the canal was filled by using the Calamus dual 3D obturation system (DENTSPLY International, Inc., Tulsa) (Figure 4), and the patient was referred to the prosthodontic department for final restoration.
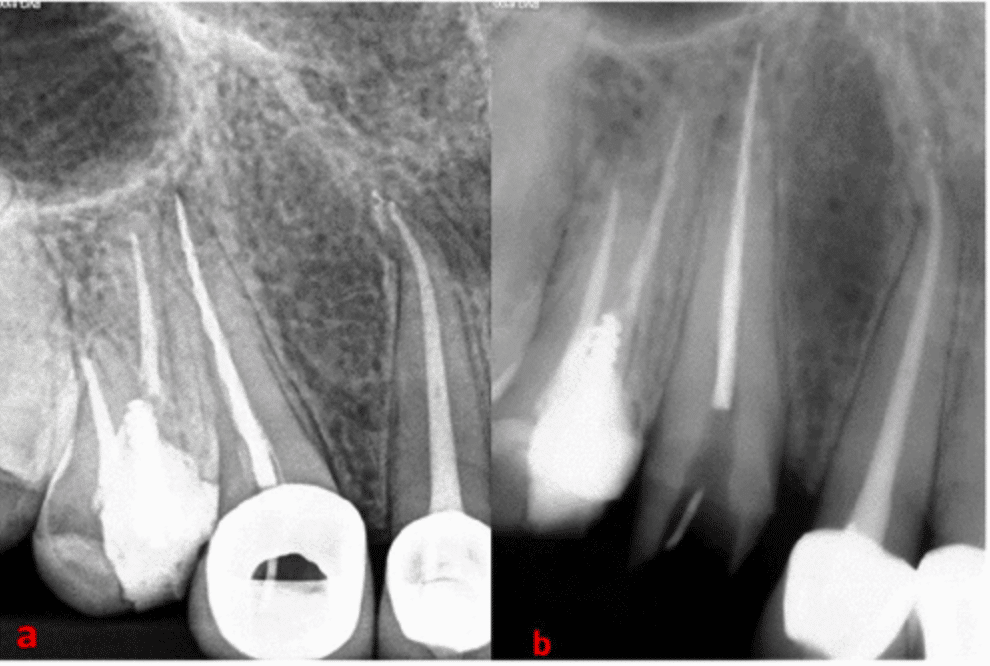
Figure 1: Diagnostic radiography (a) before and (b) after removal of the metal ceramic crown.

Figure 2: (a) Etching needle with a K file as an extraction device and (b) etching needle engaged around the separated instrument and interlocked with the K file.
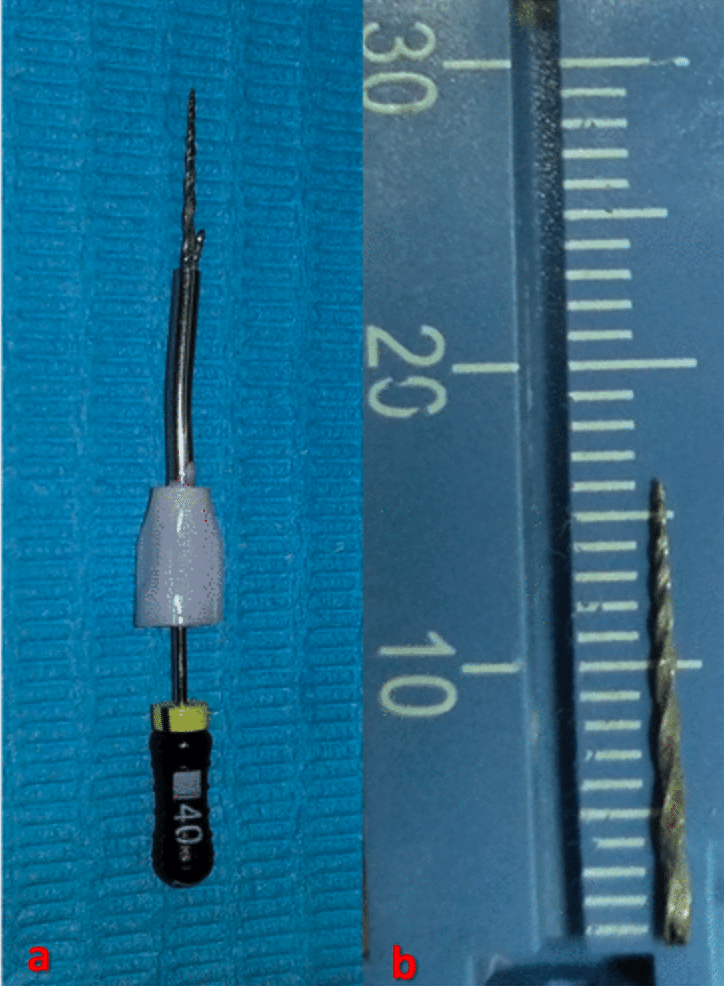
Figure 3:. Separated instrument after it was removed from the canal. (a) the removed separated instrument by hollow tube–based extractor and (b) the length of the fragment was approximately 16 mm.

Figure 4: Final root canal obturation.
DISCUSSION
Separation of an intracanal instrument is a problem that may be encountered during root canal treatment and sometimes even with routine cases.10 NiTi instruments rarely exhibit visual signs of deformation and separation without any prior warning.11 NiTi instrument separation is related to several factors such as inappropriate access cavity, curvature of the root canal, multiple uses of the same instrument, and operator experience.1,2 The use of ultrasonic tips under magnification with a dental operating microscope is considered the safest and most commonly used method to retrieve a separated endodontic instrument.2 The success rate of removal of separated endodontic instruments by using the ultrasonic tip is 80%.8 In the present case, the ultrasonic technique was attempted several times to remove the separated instrument; however, all attempts failed. The failure is likely due to the engagement of the apical part of the instrument tightly. While the present case of instrument separation was torsional separation, this type of separation occurs when the instrument (generally the tip) is locked in the canal while the file shank continues to rotate.12 In addition to the torsional fatigue separation in the present case, the large instrument size (F3) may have had a role in the instrument separation, as larger, stiffer instruments suffer from more stress during intracanal usage.12 The presence of apical periodontitis is a critical factor that has an influence on the outcome of the root canal treatment.13 The apical diagnosis of the present case was asymptomatic apical periodontitis; therefore, the removal of the separated NiTi instrument was necessary to improve the prognosis of root canal treatment. The best way to manage NiTi rotary instrument separation is to prevent the separation, and the preventive measures for NiTi instrument separation are summarized as follows:14
➢Avoid too much stress on NiTi rotary instruments during its usage;
➢Follow instructions of use for each NiTi rotary system;
➢Evaluate the root canal curvature carefully, as the probability of separation increases in cases with a severe curvature;
➢Prepare an adequate access cavity;
➢Enlarge canal orifices and prepare a glide path before using NiTi rotary instruments;
➢Always use NiTi rotary instruments with a lubricant and copious irrigation;
➢Use NiTi rotary instrument with a gentle pecking or pumping motion.
ACKNOWLEDGEMENT
We would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors of this manuscript have contributed significantly, and all authors are in agreement with the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This case report was approved by the research ethics committee of the College of Dentistry—Taibah University (Protocol no. TUCDREC/20190416/HMGhabbani) in agreement with the guidelines of the Helsinki Declaration as revised in 1975.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
ORCID iD
Mothanna K AlRahabi: https://orcid.org/0000-0001-5067-2903
REFERENCES
1. AlRahabi, M . Attitudes of general practice dentists in private dental clinics in Almadinah Almunawarah toward novel endodontic technologies. G Ital Endod 2016; 30: 10–13.
2. Fu, M, Zhang, Z, Hou, B. Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod 2011; 37(5): 619–622.
3. AlRahabi, M . Comparative study of root-canal shaping with stainless steel and rotary NiTi files performed by preclinical dental students. Technol Health Care 2015; 23(3): 257–265.
4. Hubscher, W, Barbakow, F, Peters, OA. Root-canal preparation with FlexMaster: canal shapes analysed by micro-computed tomography. Int Endod J 2003; 36(11): 740–747.
5. Di Fiore, PM, Genov, KA, Komaroff, E, et al. Nickel-titanium rotary instrument fracture: a clinical practice assessment. Int Endod J 2006; 39(9): 700–708.
6. Iqbal, MK, Kohli, MR, Kim, JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod 2006; 32(11): 1048–1052.
7. McGuigan, M, Louca, C, Duncan, H. Clinical decision-making after endodontic instrument fracture. Br Dent J 2013; 214(8): 395–400.
8. Shahabinejad, H, Ghassemi, A, Pishbin, L, et al. Success of ultrasonic technique in removing fractured rotary nickel-titanium endodontic instruments from root canals and its effect on the required force for root fracture. J Endod 2013; 39(6): 824–828.
9. AlRahabi, M, Gabban, H. Management of foreign object in the root canal of central incisor tooth. Saudi Endodontic Journal 2014; 4: 154–157.
10. Ungerechts, C, Bardsen, A, Fristad, I. Instrument fracture in root canals-where, why, when and what? A study from a student clinic. Int Endod J 2014; 47(2): 183–190.
11. Peng, B, Shen, Y, Cheung, G, et al. Defects in ProTaper S1 instruments after clinical use: longitudinal examination. Int Endod J 2005; 38(8): 550–557.
12. McGuigan, M, Louca, C, Duncan, H. Endodontic instrument fracture: causes and prevention. Br Dent J 2013; 214(7): 341–348.
13. Parashos, P, Messer, HH. Rotary NiTi instrument fracture and its consequences. J Endod 2006; 32(11): 1031–1043.
14. Di Fiore, PM . A dozen ways to prevent nickel-titanium rotary instrument fracture. J Am Dent Assoc 2007; 138(2): 196–201; quiz 249.










