

HOW DO WE KNOW THE MAJOR CONNECTOR WE NEED TO USE IN OUR RPD DESIGN?
As we all know the main role of a major connector is to unify and stablize all of the major parts of the prosthesis. It serves as a stress distributor aiding the denture base and retainer. It functions as a support, distributing masticatory forces to avoid damage and stress on soft tissues and teeth.
Since there are a lot of different types of major connectors that can be used in designing, it is essential we know the major connector that best suits our specific cases. How will we know? On this post we will review the functions, requirements, indications and types of major connectors that we can use in designing our RPD. This will refresh your knowledge and aid in knowing what's best for your Prosthodontic case.
I. FUNCTIONS OF MAJOR CONNECTORS
A. Unification
A major connector unites all other components of a partial denture so that the partial denture can act as one unit.
B. Stress Distribution
➢All elements of a partial denture, the major connector should distribute the functional loads of all abutment teeth, thus, no abutment is subjected to extreme loading.
➢The unification of the direct retainers with the denture base aids in distributing forces both the teeth and the mucosa. In some maxillary cases, a major connector with broad palatal contact is selected. In this situation, the broad base offers additional support in distributing stress over a larger area.
C. Cross-Arch Stabilization (Counter-Leverage)
By uniting one side of the arch to the other bracing elements on one side of the arch can aid in providing stability to the other. This can dissipate the twisting and torquing forces present.
II. REQUIREMENTS OF A MAJOR CONNECTOR
A. Rigidity
Rigidity is necessary to ensure that the partial denture functions as one unit. If the denture flexes, stress distribution and cross arch stabilization can be compromised since different portions of the denture can move independent with the other components. A major connector can be made more rigid by:
➢Using alloys such as chrome-cobalt; gold alloys; cast wrought metal
➢By increasing the bulk as the length increases
➢Altering the linguo-plate or rugae areas
B. Non-Interference with the Soft Tissues
➢Major connectors should not interfere into undercut areas because it is possible that movement of the connector can cause tissue impingement that can compromise blood flow. Undercuts can also cause tissue impingement. These conditions can be avoided by changing your selected path of insertion or undercut. In addition, it is best that the connectors should not end on the crest of rugae or at the free gingival margin to avoid these untoward effects.
➢Major connectors should be placed as far as the free gingival margin as possible. This is necessary to cross the gingival margin (i.e. with a minor connector) and perpendicular to the margin. Moreover, a small amount of relief is used over the area where crossing occurs in order to minimize impingement. Other areas of potential tissue impingement are the various hard structures such as the mid-palatal suture or mandibular tori, wherein it is necessary to cross these areas for denture relief, so that, the connector does not fulcrum nor interfere during the movement of the oral cavity.
C. Food Impaction
This can be minimized by locating the margins of the connectors at the prescribed distance from the free gingival margin and by taking care the presence of minor connectors, clasp arms and major connectors do not create "traps" or large concavities where food can get collected.
D. Unobtrusive
The margins of the major connector should have a smooth transition from connector to tissue so as to minimize the obtrusiveness. All line angles and edges should be smooth and rounded. Borders should not be placed in locations where they might interfere with speech. Bulk should be reduced enough so as not to interfere with speech or appearance, yet thick enough to ensure rigidity.
III. KNOWING MANDIBULAR MAJOR CONNECTORS
A. Lingual Bar
This is the most commonly used mandibular major connector. It should be used whenever possible unless there are advantages that can be obtained from another connector.
1. Shape
➢ Flat on tissue side
➢ Convex or tear-drop on tongue side (1/2 pear shape with thin edge toward teeth)
2. Size
➢ Occluso-gingival width = 4 to 6 mm
➢ Thickness = 1.5 to 2 mm
3. Position
➢ The inferior border should be as low as the lingual frenum and tissue reflections of the floor of the mouth will permit. This is determined by observing functional movements of the tongue.
➢The superior border should be 1.5-2.0 mm or more below the free gingival margin. For hygienic reasons the superior border should still be kept as far from the gingival margin as possible.
➢In distal extension cases, there will be some tissue-ward movement of the lingual bar as the denture base moves during function. If bone loss occurs over the edentulous ridges, this movement can become more pronounced and this will cause the lingual bar to impinge upon the lingual tissues. To eliminate the lingual bar from impinging the soft tissues, a wax spacer (relief) of one thickness of 30 gauge wax is placed under the major connector when it is being waxed for casting.
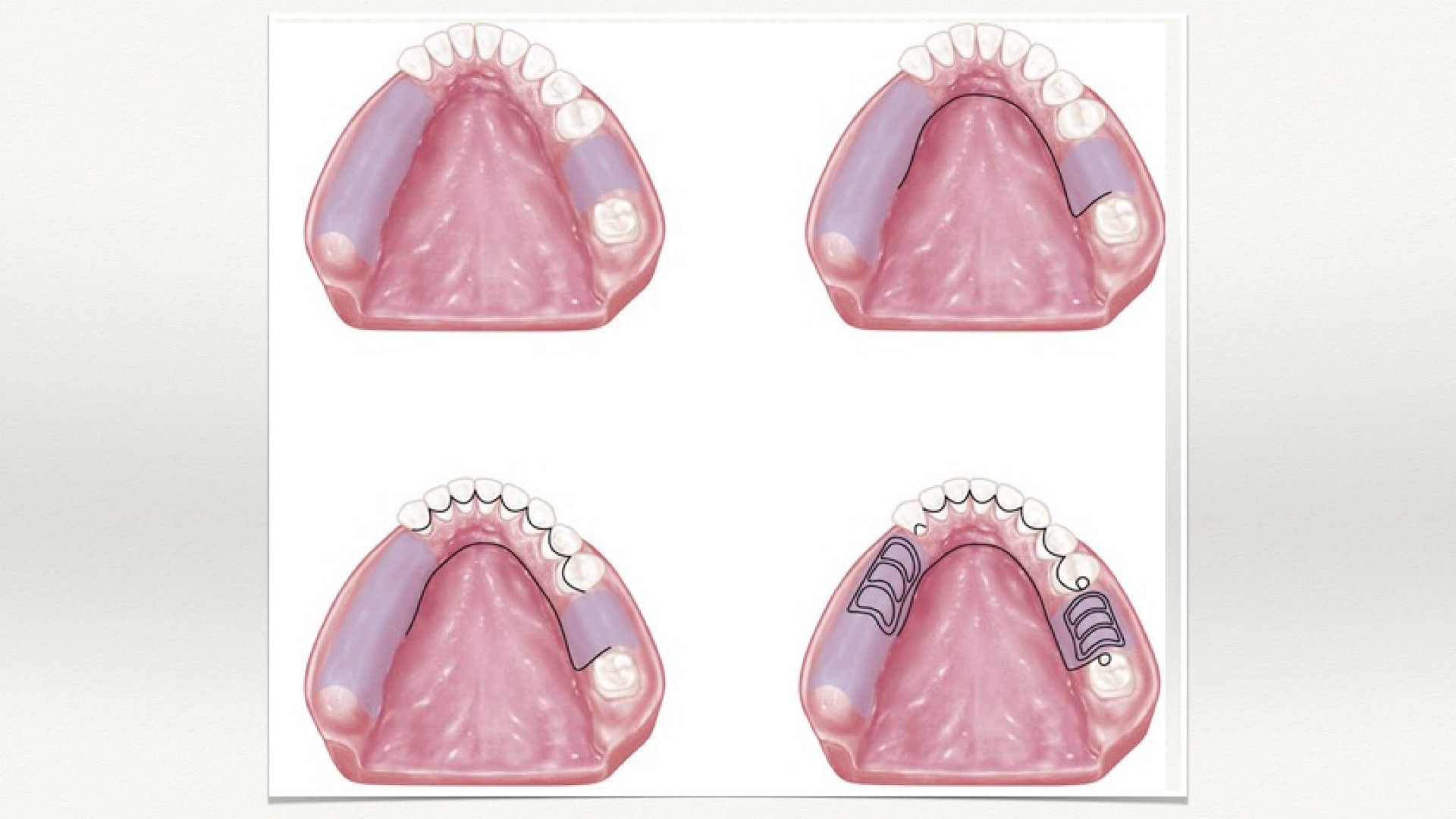
B. Lingual Plate (Linguoplate)
The lingual plate consists of a lingual bar plus an extension over the cingula of anterior teeth. This mandibular major connector should only be considered in those rare instances where a lingual bar cannot be used. Most often, this occurs when there is a high floor of the mouth, a prominent lingual frenum or lingual tori that would be impinged upon by a lingual bar, if it was made with adequate height and distance from the free gingival margin.
The lingual plate has also been advocated for extensive distal extension cases with severe vertical resorption of ridges (i.e. little resistance to horizontal rotational tendencies). In these cases the major connector could provide some additional stability. The lingual plate has been advocated for use to reduce heavy calculus formation or to stabilize mobile anterior teeth. However, the plate usually does not reduce mobility, other than stabilizing the teeth during function. Mobility per se is not a problem unless it is increasing (i.e. pathological conditions). Since mobility is often related to periodontal bone loss and since the plate complicates hygiene by closing the lingual opening of the embrasure spaces, this connector actually may be contraindicated when mobile teeth are present. When large diastema is present, the lingual plate may show through the embrasure spaces. A vertical stop or rest area must be prepared at each end of the anterior segments of the lingual plate. This prevents excessive forces being directed facially by movements of the distal extension base. Any areas where the connector crosses the gingival tissue must be relieved to prevent impingement caused by the movement of the lingual plate.
C. Labial Bar
Where extreme lingual inclination of the remaining teeth is present and no reasonable way exists to use a lingual bar without interfering with tongue movements, a labial bar may be used. It is essentially similar to the lingual bar and the same rules apply for its use. Indications for this is extremely rare. The swing-lock design is a variation of the labial bar.
IV. KNOWING MAXILLARY MAJOR CONNECTORS
Major connectors in the upper arch should terminate 4.0 mm or more from the gingival crest tissues.

A. Anterior-Posterior Palatal Strap
The anterior-posterior palatal strap provides maximum rigidity and minimum bulk. The strength of this connector lies in the fact that the anterior and posterior sections are joined together by longitudinal connectors on either side. Each component braces the other against possible torque and flexural force. It can be used in most maxillary partial denture designs and is especially useful in cases with a torus palatinus.
The double palatal strap variation is the anterior-posterior palatal bar connector where the palatal connector elements are narrower anterio-posteriorly. Due to the narrowness of the elements, the bars must have greater bulk for rigidity, and thus the design is more objectionable to the patient. In addition, strap connectors provide greater distribution of stresses to the palatal tissues since a greater surface area is contacted.
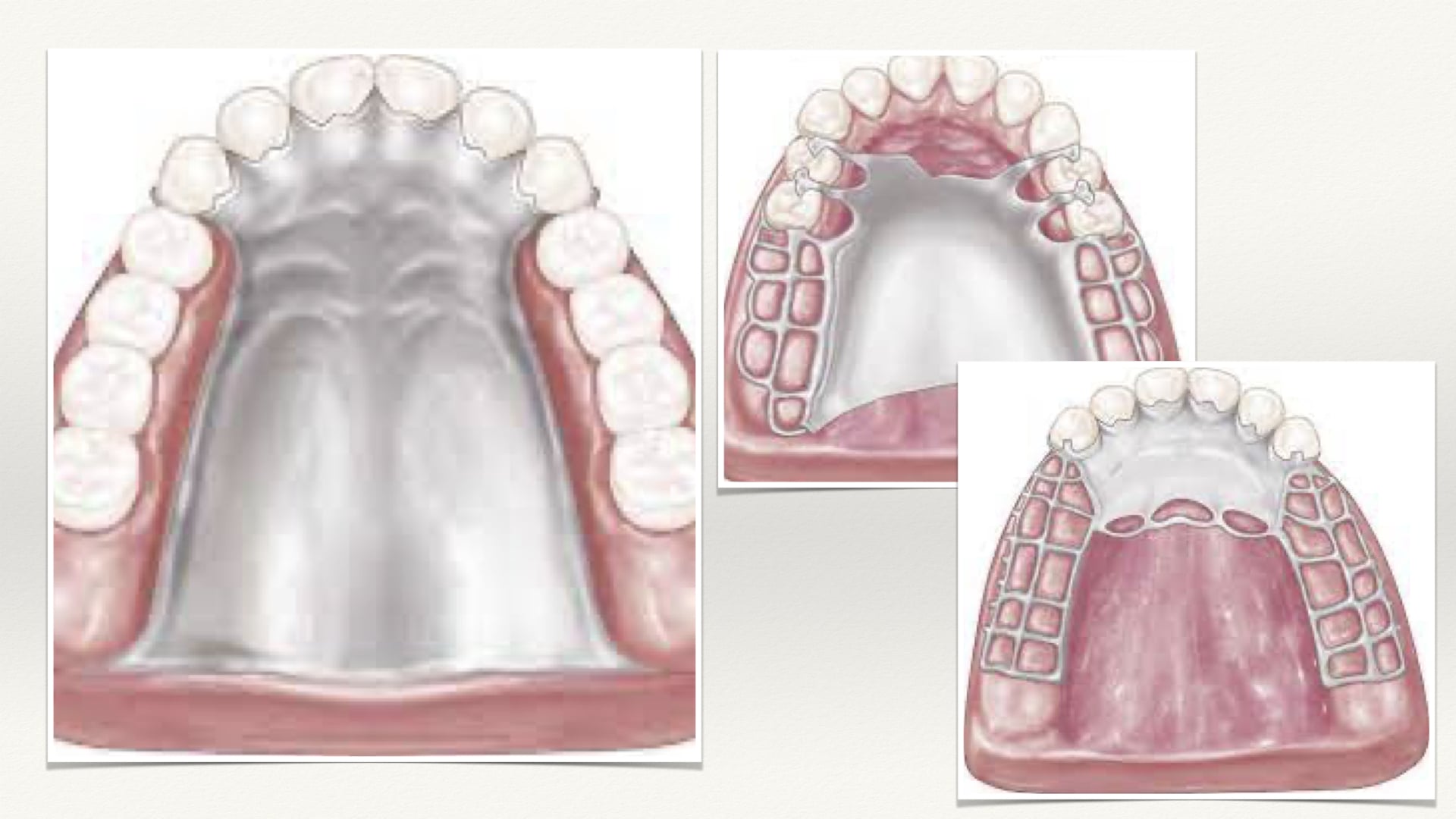
B. Full Palatal Plate
The full palatal plate is particularly indicated when maximum tissue support is required. In particular it should be the major connector of choice in long distal extension cases or where six or less anterior teeth remain. It should be selected where the primary abutments are periodontally involved, requiring maximum stress distribution. Where the edentuluous areas are covered with flabby tissue or where there is a shallow palatal vault. This connector also provides greater stability and stress distributing characteristics. The full palatal plate is usually not used in the presence of torus palatinus.
The full palatal connector should be fabricated of a uniformly thin metal plate with accurate anatomic reproduction of the rugae configuration (improves strength and rigidity). It should cover the same area posteriorly as a complete denture . The large surface area of contact with the mucosa improves the potential for retention. Connectors of this type are generally of cast metal. However, an acrylic resin plate may be used in interim prostheses.
C. Palatal Strap (or Bar)
This type of connector can be wide (strap) or narrow (bar) depending upon its location or the need for strength or support of the denture. The palatal bar should only be used in tooth supported cases where no other connector can be used. It is usually objectionable due to its bulk. It should never be used in cases involving distal extensions or replacement of anterior teeth since it must be made bulky for rigidity.
The palatal strap is similar, but, with a broader area of contact, providing better stabilization and stress distributing properties with minimum bulk. Therefore, it is preferable to the palatal bar for posterior tooth supported cases. However, other connectors should be chosen if there is a large torus or if many teeth are being replaced.
Relief may be required over bony midline areas and in some instances in order to prevent fulcrum over the overlying soft tissue. In these cases, one thickness of 28 gauge wax relief should be placed over the midline.
D. Anterior Palatal Plate (U-Shaped Or "Horse-Shoe" Palatal Connector)
From a biomechanical standpoint the palatal horseshoe is a poor connector and should never be used unless absolutely necessary. To be rigid, the horseshoe connector must have bulk in the rugae area where the tongue requires freedom. Without sufficient bulk the U-shaped design becomes flexible and allows movement posteriorly. In distal extension partial dentures where posterior tooth support is nonexistent, movement is particularly noticeable and is traumatic to the residual ridge causing continual irritation during function. The anterior palatal plate should only be prescribed where the torus palatinus prohibits the use of other connectors. It is also important that soft tissue movements during function must also be allowed especially the mandibular lingual frenum and the maxillary movable soft palate.
CONCLUSION
By familiarizing with the designs of a removable partial denture, we, as dentist can make careful examination of the mouth to ensure the selected major connector will not interfere with any soft tissue structures. These indications would help achieve the optimal comfort and function for our patients.
CONTRIBUTORS:
Dr. Bryan Anduiza - Writer
Dr. Mary Jean Villanueva - Editor










