

HOW DO WE DESIGN OUR RPD THAT CAN PROVIDE STABLE RETENTION?
Before we dive into this topic, you might like to start and read first our other previous removable partial denture posts: “Removable Partial Denture: Review On Its Classification”: READ
And, ”RPD Major Connectors Review”: READ
One the most significant functionalities of a denture is its ability to provide good retention. Retention as we know is defined as the ability of a removable partial denture to resist dislodging forces during functions such as speech and mastication.
The retention needed depends on several factors:
a. Adhesion, cohesion, interfacial surface tension and atmospheric pressure.
b. Gravity
c. Frictional retention (guiding planes, bracing elements)
e. Indirect retention
f. Direction of dislodging force relative to the path of placement.
g. Mechanical retention
The latter function, which is mechanical retention, is obtained by placing portions of the partial denture into tooth or soft tissue undercuts. And, majority of mechanical retention is derived from the use of direct retainers or clasp assemblies utilizing tooth undercuts.
For even better understanding, let’s define and differentiate 2 important terms:
Direct Retention is the retention obtained in a RPD by the use of clasps or attachments that resist removal from the abutment teeth.
Direct Retainer is that component of RPD used to retain and prevent dislodgement consisting of a clasp assembly or precision attachment such a manner as to resist displacement of the prosthesis away from the soft tissue. It is usually composed of a retentive arm, a reciprocal (bracing) element or arm, a rest and a minor connector.
With different designs, the direct retainers of removable partial dentures have different effects on stability of abutment teeth and retention of removable partial denture. This post serves as a review for different retainers used in designing. It discusses each advantages and disadvantages when applied on different Kennedy classification.
REQUIREMENTS OF A CLASP ASSEMBLY
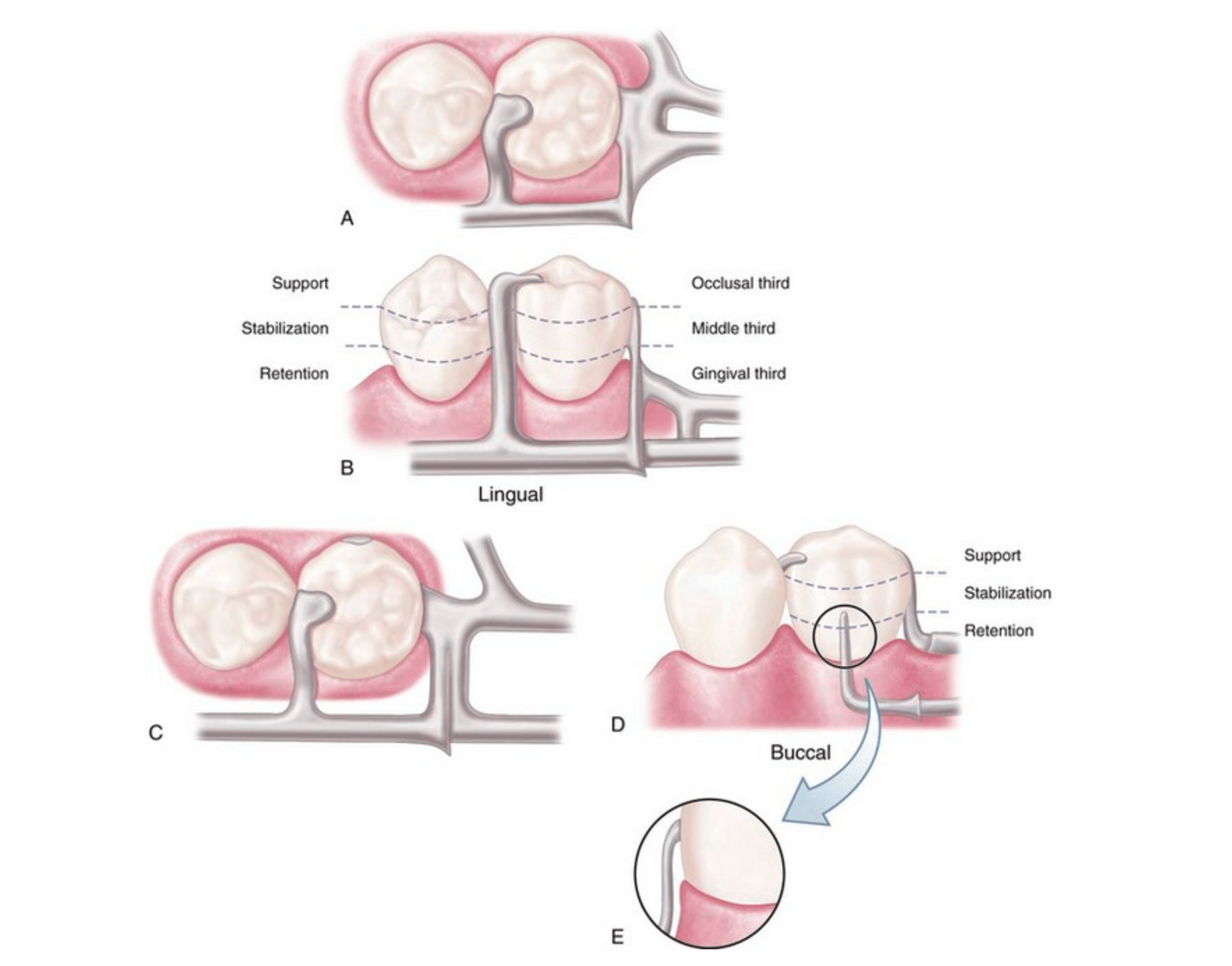
Bar-type clasp assembly. A, Occlusal view. Component parts (proximal plate minor connector, rest with minor connector, and retentive arm) tripod the abutment to prevent its migration. B, The proximal plate minor connector extends just far enough lingually so that it combines with the mesial minor connector to prevent lingual migration of the abutment. C, On narrow or tapered abutments (mandibular first premolars), the proximal plate should be designed to be as narrow as possible but still sufficiently wide to prevent lingual migration. D, I-bar retainer located at greatest prominence of tooth in the gingival third. E, Mesial view of I-bar illustrating the retentive tip relationship to the undercut and a region superior to the height of contour, which serves a stabilization function in encirclement.
These factors should be found to be able to be classified as direct retainer:
1. Support - the retainer should be able to provide resistance to gingival displacement (occlusal rests).
2. Reciprocity - the retainer should be able to provide resistance to orthodontic movement of teeth using reciprocal arms or elements placed against guiding planes. During placement and removal of the partial denture the retentive arm flexes over the height of contour and generates energy. At this point the rigid reciprocal arm should contact the guiding plane and prevent orthodontic movement from taking place.
3. Stability - the retainer should be able to provide resistance to lateral movement (reciprocal arms, minor connectors)
4. Retention - the retentive arms should be located in undercuts on the abutments.
5. Encirclement of Greater than 180° of the Tooth - the clasp arms should prevent the prosthesis from moving away from the tooth.
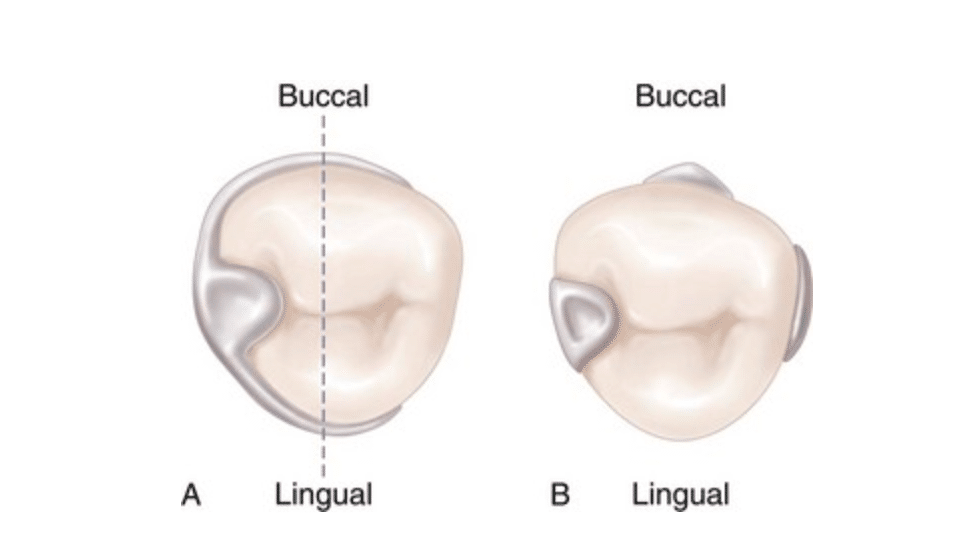
A. Line drawn through the illustration represents 180 degrees of greatest circumference of abutment from the occlusal rest. Unless portions of the lingual reciprocal arm and the retentive buccal arm are extended beyond the line, the clasp would not accomplish its intended purpose. If respective arms of the retainer were not extended beyond the line, the abutment tooth could be forced away from the retainer through torquing action of the clasp, or the removable partial denture could move away from the abutment. B. Bar-type clasp assembly engagement of more than 180 degrees of circumference of the abutment is realized by the minor connector for the occlusal rest, the minor connector contacting the guiding plane on the distal proximal surface, and the retentive bar arm.
6. Passivity - when the oral cavity is at a resting position, the direct retainer should not exert force against a tooth.
CLASSIFICATION OF DIRECT RETAINERS
I. Intracoronal Retainers
These are mechanical devices used in RPD that wants to balance between functional stability and cosmetic look in RPD. For these goals there are 2 Classifications of Attachments that were developed based on method of fabrication and the tolerance of fit:
A. Precision Attachments
➢Are very precise, and are milled out of alloy. The male and female parts fit together with tolerances of about 10 microns. They are purchased as a finished product and are soldered or cast to the final prosthesis. They are incorporated within the contours of the crown or splint and direct the forces of occlusion down the long axis of the tooth. They are generally rigid attachments in that the prosthesis is able to transfer most of the occlusal force to the teeth in which the attachments are incorporated, and less to the tissue-bearing areas.
Indication | Application of Precision Attachments Removable Prosthodontics:
➢ As a retainer in a removable tooth supported partial denture 4 large well rounded abutments are available For esthetic concern in the anterior part of the mouth.
➢ Stress Breakers – Free end Saddles or Distal Extension Base cases (DEB) – When cantilevered pontic is to be used as abutment.
➢ For movable joints in sectional dentures.
➢ Periodontal involvement of the tooth the contraindicates rigid FPDs.
➢ Most efficient bilateral bracing and support are essential.
Contraindications of Precision Attachments:
➢ Poor periodontal support.
➢ Poor crown to root ratio.
➢ Poor oral hygiene habits.
➢ Abnormally high carious rate.
➢ Inadequate space or room to employ the attachment.
➢ Compromised endodontic and restorative conditions.
B. Semi-Precision Attachments
➢Are much less precise in their fit and usually have much more resiliency than their precision attachment counterparts. These attachments are cast from refractory patterns, and the male or female parts may be made of nylon, polymer, or metal. These attachments can allow up to 15 degrees (or more) of rotational movement and up to 600 microns (or more) of vertical movement. Some offer hinge and/or lateral resiliency. In removable partial denture cases, they are cast with the crown or splint and are placed outside the contours of the teeth. In overdenture prosthetics, they are either cast on top of copings, incorporated onto posts which are cemented into the roots or abutment teeth or incorporated into overdenture implant abutments. Their resiliency allows the prosthesis to transfer most of the occlusal load to the tissues and away from the abutment teeth to which they are connected.
II. Extracoronal Retainers
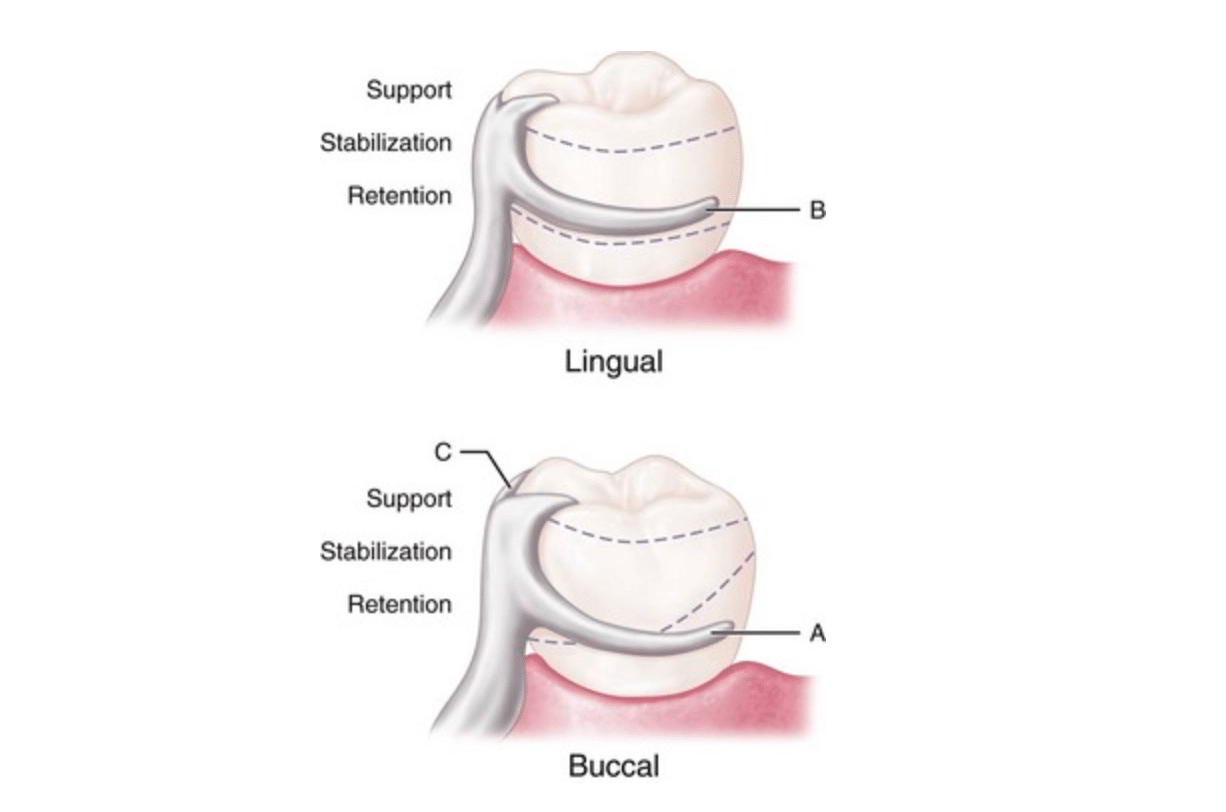
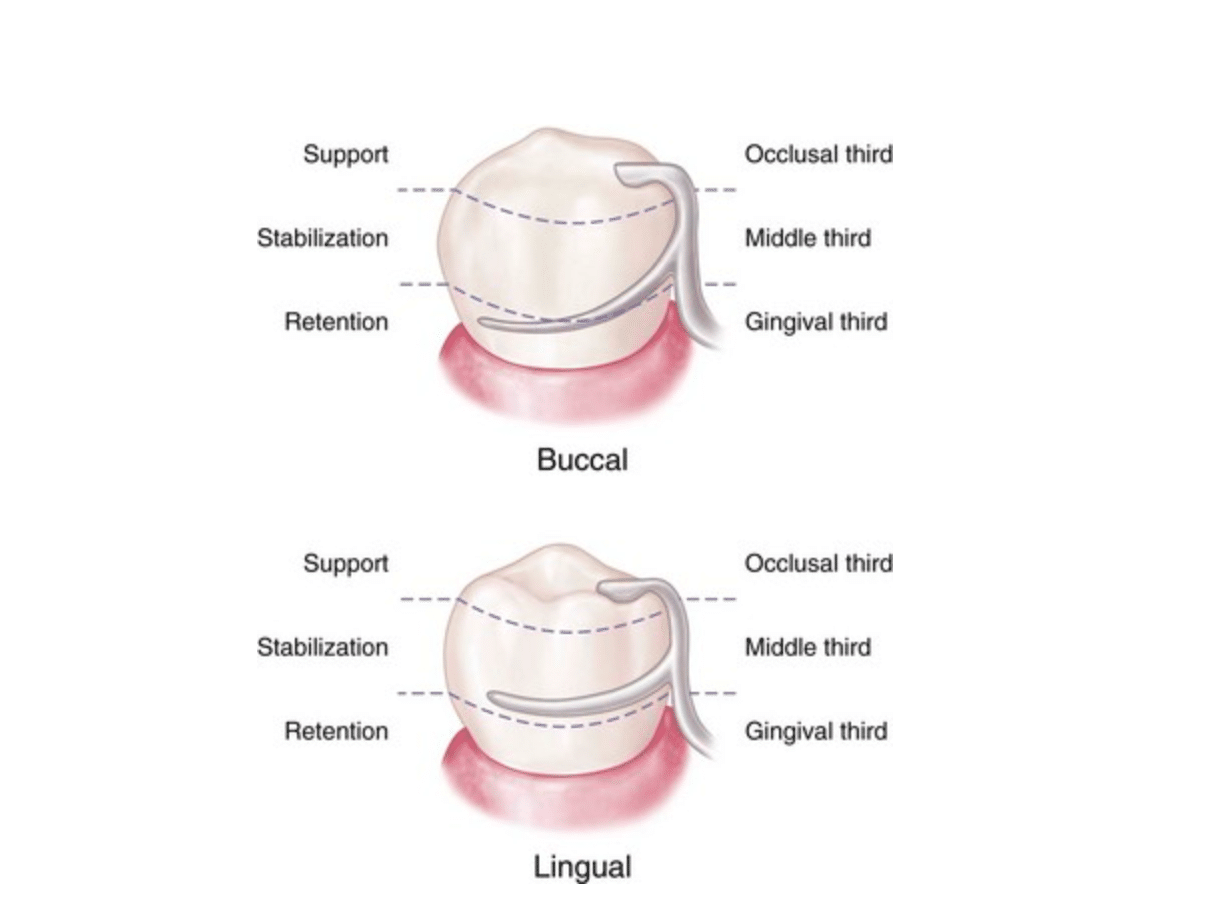
Extracoronal circumferential direct retainer. Assembly consists of (A) the buccal retentive arm; (B) the rigid lingual stabilizing (reciprocal) arm; and (C) the supporting occlusal rest. The terminal portion of the retentive arm is flexible and engages measured undercut. Assembly remains passive until activated by placement or removal of the restoration, or when subjected to masticatory forces that tend to dislodge the denture base.
➢Engage an external surface of an abutment in a natural undercut or in a prepared depression. There are two main classes:
A. Retentive Clasp Assemblies
➢This is categorized into 2 types by MM Devan:
(1) Suprabulge Retainers - those that approach the undercut from above the height of contour or that portion of an abutment that converges towards the occlusal or incisal surface and is considered as supra bulge aspect of the abutment.
(2) Infrabulge Retainers - those that approach the undercut from below the height of contour or that portion of the clinical crown that converges apically from the height of contour and is considered the infrabulge aspect of the abutment.
B. Extracoronal Attachments
➢ This means that the attachment is located outside the teeth.
➢ This was first proposed in 1900 by Henry H. Boss and later modified by Ewing F. Roach in 1908.
➢ The retention comes from closely fitting components termed matrices and patrices.
➢ This permit vertical movement during occlusal loading, minimizes potentially damaging forces to abutment. This concept has led to “stress breaking” or “stress directing” theories of RPD.
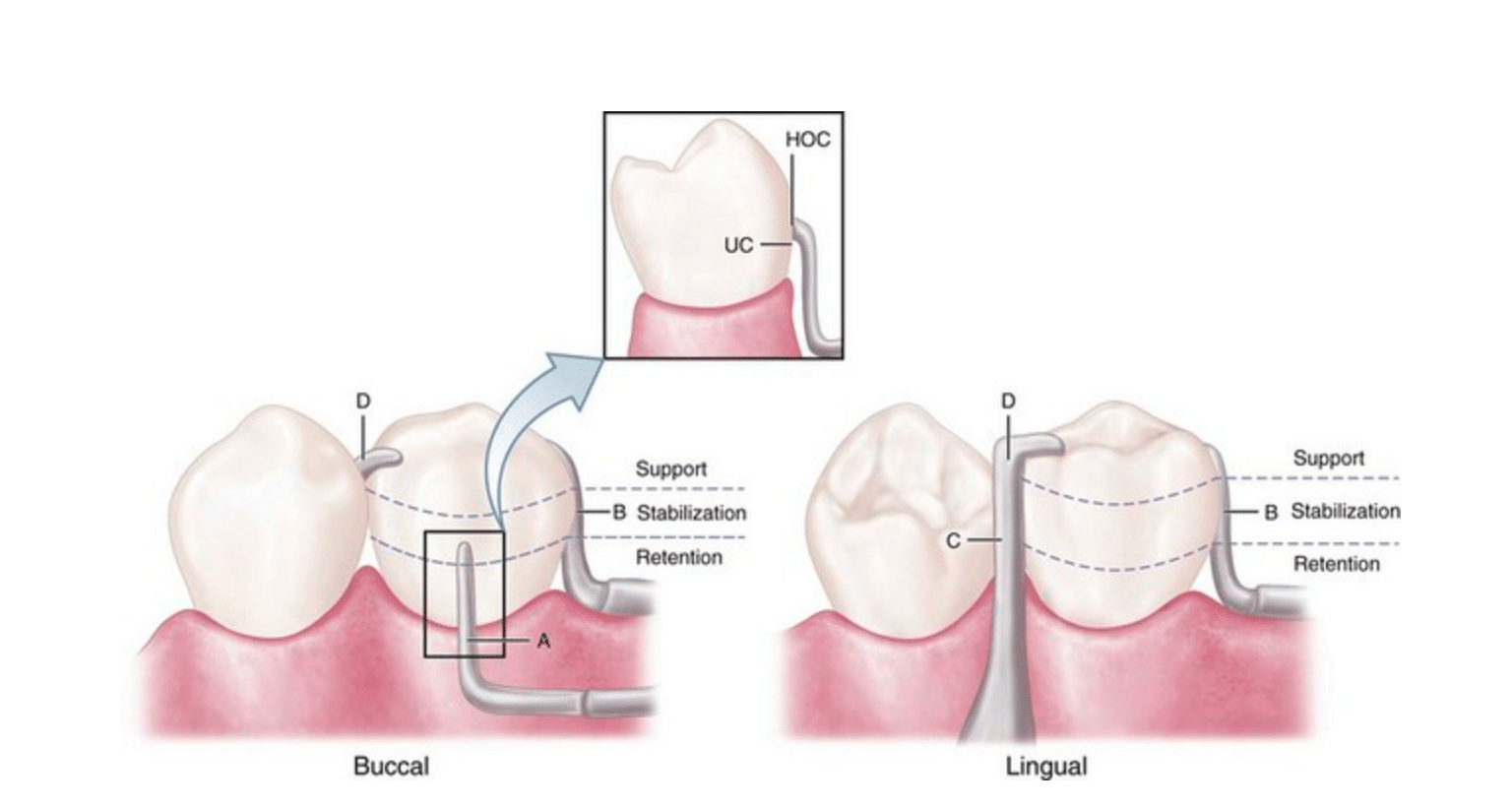
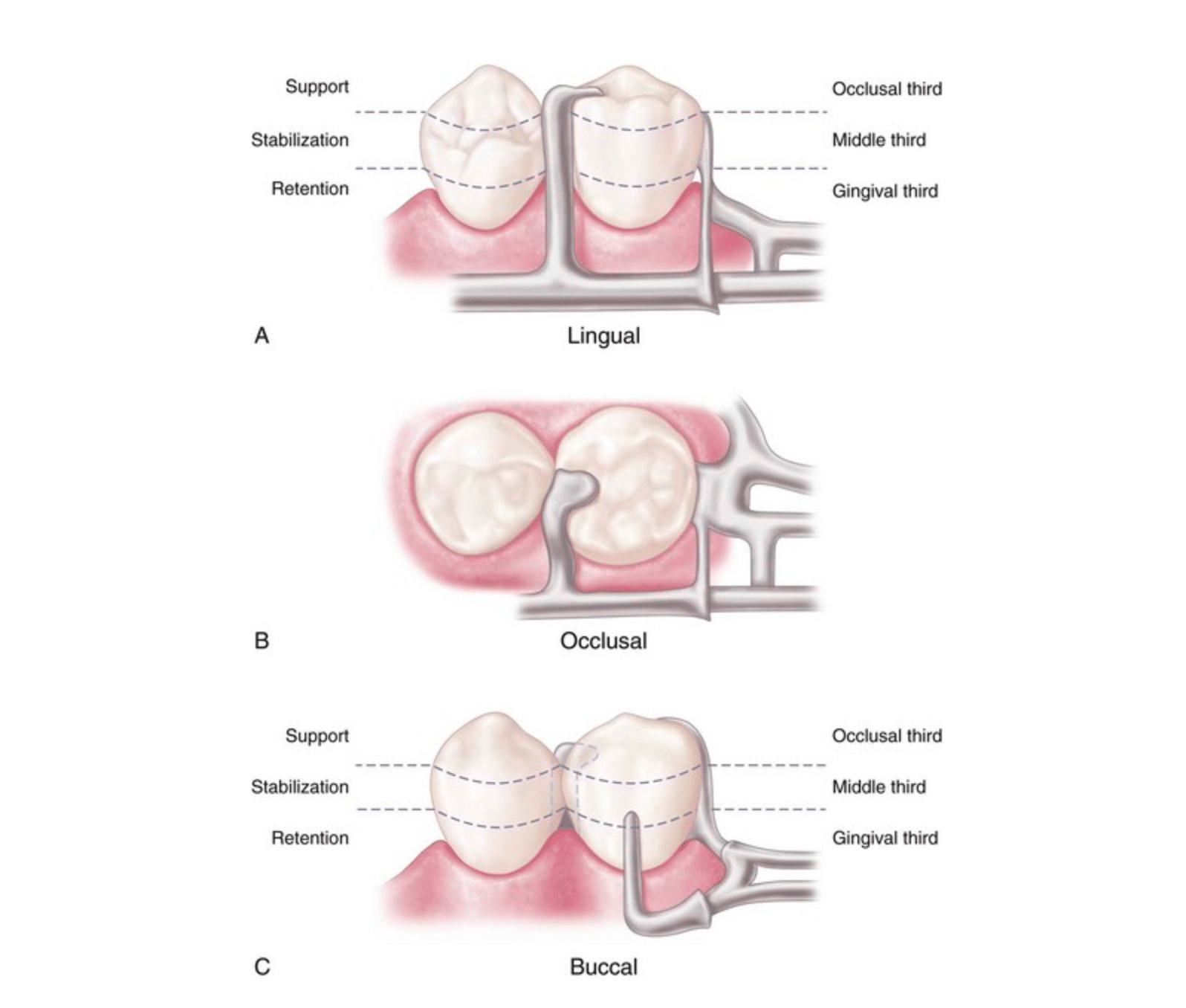
Extracoronal bar-type direct retainer. Assembly consists of (A) the buccal retentive arm engaging the measured undercut (with slight occlusal extension for stabilization, see insert where HOC is height of contour and UC is undercut); (B) the stabilizing (reciprocal) elements, with the proximal plate minor connector on the distal; (C) the lingually placed mesial minor connector for the occlusal rest, which also serves as a stabilizing (reciprocal) component; and (D) the mesially placed supporting occlusal rest. Assembly remains passive until activated.
TYPES OF CLASPS FOR TOOTH BORNE RPD
These are examples of Direct retainers used for tooth-borne partial dentures that belong to (Kenedy Class III, IV). Their main function is to prevent dislodgment of the prosthesis without damaging the abutment teeth and other tissue surface. Since there is little or no rotation caused by tissue movement of the edentulous area (as happens in distal extension cases) stress releasing properties are usually not required. These clasps can also be used in modification spaces for tooth and tissue supported removable partial dentures (Class I, II).
I. Circumferential (Circle or Akers) Clasp
Circumferential clasp on the mandibular premolar. Support is provided by the occlusal rest; stabilization is provided by the occlusal rest, proximal minor connector, lingual clasp arm, and rigid portion of the buccal retentive clasp arm occlusal to the height of contour; retention is realized by the retentive terminal of the buccal clasp arm; reciprocation is provided by the nonflexible lingual clasp arm. Assembly engages more than 180 degrees of the abutment tooth’s circumference.
Design:
(a) The class should arise from the main body of the clasp assembly above the height of contour.
(b) All the components of the C clasp should be present above the height of contour except the retentive tip.
(c) The retentive terminus should always be directed towards the occlusal surface never towards the gingiva
(d) It should always terminate at the mesial or distal line angle never at midfacial or midlingual surface.
INDICATIONS:
➢ Tooth supported partial denture.
CONTRAINDICATIONS:
➢ It is not ideal for distal extension cases as they engage the mesiobuccal undercut.
ADVANTAGES:
(a) Excellent bracing, support and retentive qualities.
(b) Easy to design and construction
(c) Less potential for food accumulation due to close adaptation to the tooth surface.
DISADVANTAGES:
(a) More tooth coverage than bar clasps.
(b) More metal is displayed than with bar or combination clasps.
(c) Adjustments are difficult or impossible due to the half round nature of the clasp
II. Ring Clasp
DESIGN:
(a) Ring clasp as type of retainers that encircles nearly the entire abutment tooth. Found usually used with mesially and lingually tilted mandibular molars (with a m-l undercut) or mesially and buccally tilted maxillary molars (with a m-b undercut)
(b) The undercut is on the same side as the rest seat (i.e. adjacent to edentulous span).
(c) Clasp should always be used with a supporting strut on the non-retentive side with an auxiliary occlusal rest on the opposite side. Omission of the supporting strut will allow the clasp arm to open and close with minimum or no reciprocation.
INDICATIONS:
➢ Tooth supported partial denture.
➢ Tipped mandibular molars.
CONTRAINDICATIONS:
➢ Excessive tissue undercuts prevent the use of a supporting strut.
➢ Limited vestibular depth precludes placement of an auxiliary bracing arm.
ADVANTAGES:
(a) Excellent bracing and adequate encirclement.
(b) Allows use of an available undercut adjacent to edentulous area.
(c) Excellent retention with adequate flexibility due to increased length of clasp arm.
DISADVANTAGES:
(a) Covers a large area of tooth surface, thus, require meticulous hygiene.
(b) Very difficult to adjust due to the extreme rigidity of the reciprocal arms.
(c) The lower bracing arm should be at least 1 mm from the free gingival margin and relieved to prevent impingement of the gingival tissues.
(d) Decalcification of teeth.
(e) Poor structure of clasp.
(e) Susceptible to distortion and fracture.
III. Embrasure (Double Akers) Clasp
DESIGN:
(a)Two circlet clasps joined at the body. Two rests, two retentive arms, and two bracing arms.
(b) Frequently used on the side of the arch where there is no edentulous space or where a distal approach clasp cannot be used on the most posterior tooth (i.e. No usable retentive undercut).
(c) Occlusal rests must be used to support the embrasure portions of the clasp. Double rests with definite shoulders to prevent weakening of clasp arms, separation of teeth and food impaction.
(d) Buccal and lingual proximal areas must be opened (i.e. Blend with axial contours, reduce height of contours, round occluso-axial line angles).
(e) Wedging of the abutments can also occur if rest seat preparations are inadequate or omitted.
(f) The rest seat preparations must be deeper toward the center of the occlusal surface than at the marginal ridges.
INDICATIONS:
➢ Tooth supported partial denture.
CONTRAINDICATIONS:
➢ Prone to distortion when there’s a use of minimum retention.
ADVANTAGES:
➢ Allows placement of direct retainer where none could otherwise be placed (especially contralateral to the edentulous span on a Class II case)
DISADVANTAGES:
(a) Extensive interproximal reduction is usually required.
(b) Covers large area of tooth surface that may result to poor hygiene conditions.
IV. "C" Clasp (Hair-Pin or Reverse Action)
DESIGN:
(a) The retentive area (undercut) is adjacent to the occlusal rest.
(b) The upper arm is a minor connector giving rise to tapered lower arm.
(c) The retentive arm has 2 horizontal components: i. The occlusal portion - minor connector and must be rigid. ii. The apical portion - pass over the height of contour to engage the desired undercut.
INDICATIONS:
(a) Tooth supported partial denture.
(b) Used when a distofacial undercut is present adjacent to the edentulous space.
(c) When using a retentive arm there must considerations on the sufficient clinical crown height; space between occlusal and apical arm; and, occlusal arm shouldn’t interfere within the occlusion.
(d) An indication of using a retentive arm is when soft tissue contour precludes use of a bar-type clasp and when the reverse circlet cannot be considered because of a lack of occlusal clearance.
ADVANTAGES:
➢ Allows use of undercut adjacent to edentulous space
DISADVANTAGES:
(a) Almost impossible to adjust.
(b) Non-esthetic
(c) Difficult to fabricate so the upper portion of the retentive arm clears the opposing occlusion.
(d) Covers extensive tooth surface and acts as a food trap
(e) Insufficient flexibility on short crowns due to insufficient clasp arm length
TYPES OF CLASPS FOR TOOTH AND TISSUE BORNE RPD
Tooth and tissue borne situations like ( Kennedy Class I & II) require special attention in direct retainer selection, due to stresses created by rotational movements of the prostheses. When left unchecked, possible problems arise such as destruction of the abutment tooth and tissue impingement.
So, when the denture bases are placed under function, rotation occurs about the rest seats of the most posterior abutments. And, excessive occlusal forces on the distal-extension portion of the denture could cause a torquing action on the abutment teeth the type of clasps for direct retainers must be designed with stress-breaking capabilities which is why these types must be both supported by the teeth and supporting tissues. The stress releasing clasp assemblies of this nature includes the following:
I. Bar Clasps
A. bar-type clasp on the mandibular premolar. A, Support is provided by the occlusal rest. B. Stabilization is provided by the occlusal rest and the mesial and distal minor connectors. C. Retention is provided by the buccal I-bar. Reciprocation is obtained through the location of the minor connectors. Engagement of more than 180 degrees of circumference of the abutment is accomplished by proper location of components contacting the axial surfaces. (The minor connector supports the occlusal rest, the proximal plate minor connector, and the buccal I-bar.)
DESIGN:
(a) Approach arm should not impinge the soft tissues.
(b) These infrabulge retentive clasps are identified by shape of retentive terminal, i.e. T, Y, I and other retentive clasps i.e. U, and S.
(c) Tissue surface smooth and well polished.
(d) Approach arm should cross the free gingival margin at 90 degrees.
(e) To optimize flexibility the approach arm should be uniformly tapered from its origin to the clasp terminus.
(f) Clasp terminus should be positioned as far apically on the abutment as it’s practical.
(g) Infrabulge clasp approaches the undercut region of an abutment from an apical direction.
(h) L-shaped clasp is same as an I clasp with a longer horizontal component.
(i) The U-shaped clasp is same as an L-shaped clasp with a terminal like a double I-clasp.
(j) The Y-clasp is formed when the approach arm terminates in the cervical 3rd of the abutment, while the mesial and distal projections are positioned near the occlusal surface. When height of contour high on the mesial and distal line angle but lower in centre.
(k) The I clasp has a horizontal retentive tip. This retentive tip contacts the abutment surface only at the undercut region. The amount of contact is about 2 to 3mm in height and 1.5mm in width.
(l) Soft tissue relief is provided under the approach arm with 28 or 30 gauge wax, to prevent tissue impingement.
INDICATIONS:
(a) For push type retention.
(b) In need of flexibility of clasp from length and taper.
(c) For more esthetic result than a C clasp such as Y clasp, T clasp and I clasp.
(d) For T-Clasp is for Kennedy Class I and Class II partially edentulous situations when an undercut is located adjacent to the edentulous area.
(e) For modified T-clasp design is used on canines and premolars for esthetics.
(f) The S-shaped terminal end is used to avoid a mesial soft tissue undercut.
CONTRAINDICATIONS:
(a) Patients with poor oral hygiene.
(b) For T clasps, it is not ideal when the available undercut is located on the mesiofacial aspect of the most posterior abutment; if the approach arm must cross over an area of severe soft tissue undercut and when the height of contour is located near the occlusal surface.
ADVANTAGES:
(a) More clasp flexibility.
(b) More esthetic result.
DISADVANTAGES:
(a) Can result to deep cervical undercuts that causes food trap or impingement result.
(b) Severe soft tissue or bony undercuts also causes food trap or impingements result.
(c) Insufficient vestibular depth for approach arm (requires 4 mm - 3 mm from free gingival margin, 1 mm for thickness of the approach arm)
(d) Pronounced frenal attachments in area - impingement
II. The R-P-I Clasp
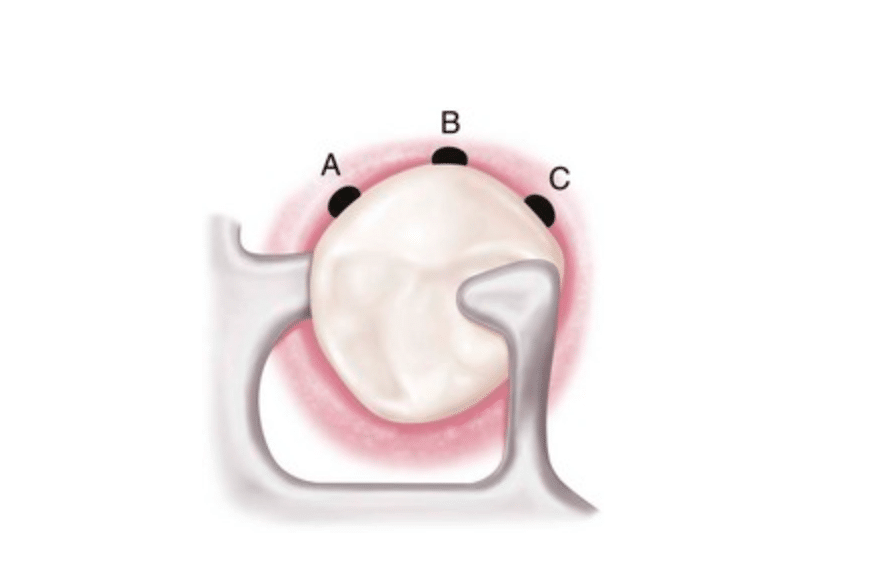
Occlusal view of the RPI (rest, proximal plate, and I-bar component parts) bar clasp assembly. Placement of the I-bar in a 0.01-inch undercut (A) on the distobuccal surface; (B) at the greatest mesiodistal prominence; and (C) on the mesiobuccal surface.
DESIGN:
(a) The components of this clasp assembly are:
"R" - Rest (always mesial)
"P" - Proximal plate
"I" - I-bar (retentive arm)
(b) The rest is located on the mesio-occlusal surface of a premolar or mesiolingual surface of a canine. The minor connector is located in the mesio-lingual embrasure but is not in contact with the adjacent tooth (prevents wedging).
(c) The proximal plate (essentially a wide minor connector) is located on a guide plane on the distal surface of the tooth. The superior edge of the proximal plate is located at the bottom of the guide plane (at approximately the junction of the occlusal and middle third of the guide plane). The proximal plate extends lingually so that the distance between the minor connector and the proximal plate is less than the mesio-distal width of the tooth. The plate is approximately l mm. thick and joins the framework at a right angle.
(d) The I-bar clasp is located on the buccal surface of the premolar and on the mesio-buccal surface of the canine. The I-bar originates at the gridwork and approaches the tooth from the gingival direction. The bend in the I-bar should be located at least 3 mm. from the gingival margin. This distance will prevent food entrapment and provide the length for the necessary flexibility in the clasp arm. The clasp is usually cast and is placed just below the height of contour line.
(e) On premolars, the proximal plate should extend lingually so that the distance between the proximal plate and the mesio-occlusal rest is less than the mesio-distal width of the tooth. The proximal plate in conjunction with the mesial rest (and minor connector) acts as the reciprocating element of the clasp and prevents the lingual migration of the tooth when the clasp arm moves over the height of contour.
(f) On cuspids, the minor connector cannot be used for reciprocation since it does not contact the tooth until after the retentive element has passed across the height of contour and the partial denture is seated. This is because the mesio-lingual rest is located fairly low on the cingulum of the tooth. Therefore, the I-bar is located in the mesio-buccal undercut and is reciprocated directly by the proximal plate.
(g) The guiding plane is a parallel surface prepared on the occlusal one third of the distal surface of the tooth. The guiding plane extends lingually enough so that, along with the mesial rest, it can prevent lingual migration of the tooth. It is approximately 2 to 3 mm in height.
CONTRAINDICATIONS:
(a) Insufficient depth of the vestibule to permit the approach arm of the I bar to be located at least 3 mm from gingival margin.
(b) A tooth which has a severe lingual tilt and no labial or no labial or buccal undercut on the abutment.
(c) Severe soft tissue undercut that the approach arm of the I bar would be too far away from the tissue and act as a food trap or irritate the mucosa of the lip or cheek.
(d) A tooth which has only a distobuccal retention undercut (less than 180° encirclement) and does not require a restoration.
(e) A mouth with a high floor in which a lingual plate is used on the lingual surface of the abutment tooth.
(f) Teeth which are severely flared labially or bucally.
III. RPA Clasp
DESIGN:
(a) This clasp assembly is similar to the RPI design except a wrought wire circumferential clasp (Akers) is used instead of the I-bar.
(b) This clasp arises from the proximal plate and terminates in the mesio- buccal undercut. It is used when there is insufficient vestibule depth or when a severe tissue undercut exists.
ADVANTAGES:
(a) The circumferential-type retentive arm is easier to grasp for removal of the prosthesis.
(b) The clasp is simple in design with few variations among patients and thus can be easily and consistently fabricated by dental laboratories.
(c) The circumferential retentive arm avoids the tissue problems around abutment teeth and allows the RPA clasp to be used in many situations where the RPI clasp is contraindicated.
IV. Combination Clasp
DESIGN:
(a) The combination clasp is similar to the cast circumferential clasp with the exception that the retentive arm is fabricated from a round wrought wire (platinum-gold-palladium alloy or chrome- cobalt alloy).
(b) A combination clasp is a cast reciprocal arm placed with a mesial or buccal undercut.
(c) Made from a flexible wrought wire than can be adjusted than cast or ½ round forms. Due to its small diameter and rounded form it presents to have better esthetics than other clasp. for best results, the wire should be soldered remotely to the framework so it is not overheated, which would cause recrystallization of the metal and loss of flexibility. If wrought wire clasps are cast into the framework, a low heat chromium alloy should be used to avoid recrystallization as well
ADVANTAGES:
➢ Can engage greater undercut.
DISADVANTAGES:
(a) More prone to breakage than cast.
(b) Minimal stabilizing.
CONCLUSION
Let's always remember that a direct retainer should be designed with its elements in the proper indication and in the correct position. Using inappropriate retainers may cause problems to you design making it less efficient in its retention or worst may damage the tooth.
CONTRIBUTORS:
Dr. Bryan Anduiza - Writer
Dr. Mary Jean Villanueva - Writer | Editor
REFERENCES
1. Stewart,Rudd and Kuebker :Clinical removable Partial Prosthodontics, 4th edition.2008.
2. McCracken’s removable partial prosthodontics, 13th Edn. St. Louis ; CV Mosby Co.
3. Krol AJ. RPI clasp retainer and its modifications. Dent Clinics North Am 1973;17:631– 649. 4. RPA clasp design- Charles Eliason – J prosthet dent:1983:49;25-27
4. Khan SB.Aesthetic Clasp Design for Removable Partial Dentures: A Literature Review. SADJ 2005 :60;5:190 – 194.
5. Zoidis P, Papathanasiou I,Polyzois G, .The Use of a Modified Poly-Ether-Ether-Ketone (PEEK) as an Alternative Framework Material for Removable Dental Prostheses. A Clinical Report. Journal of Prosthodontics.2015;1–5. 99
6. British Dental Journal, Volume 190, No. 2 January 27, 2001
7. Images credited to Pocket Dentistry: https://pocketdentistry.com










